Ovarian Tumours
Ovarian tumours in dogs and cats are very
uncommon. True reports of these tumours are unknown because most reports in
literature are based on necropsy findings. The reason behind low true clinical
evidence of ovarian tumours is large segment of canine and feline population is
surgically neutered at an early age.
Ovarian
tumours are mainly classified into three categories, according to nature of
cell origin.
· 
Epithelial cell
·
Sex cord stromal cell
Breeds which get affected in common are
Pointers, English Bulldogs, Boxers, German Shepherds, Yorkshire Terriers and
Indian Hounds.
1)
Epithelial Cell Tumours-
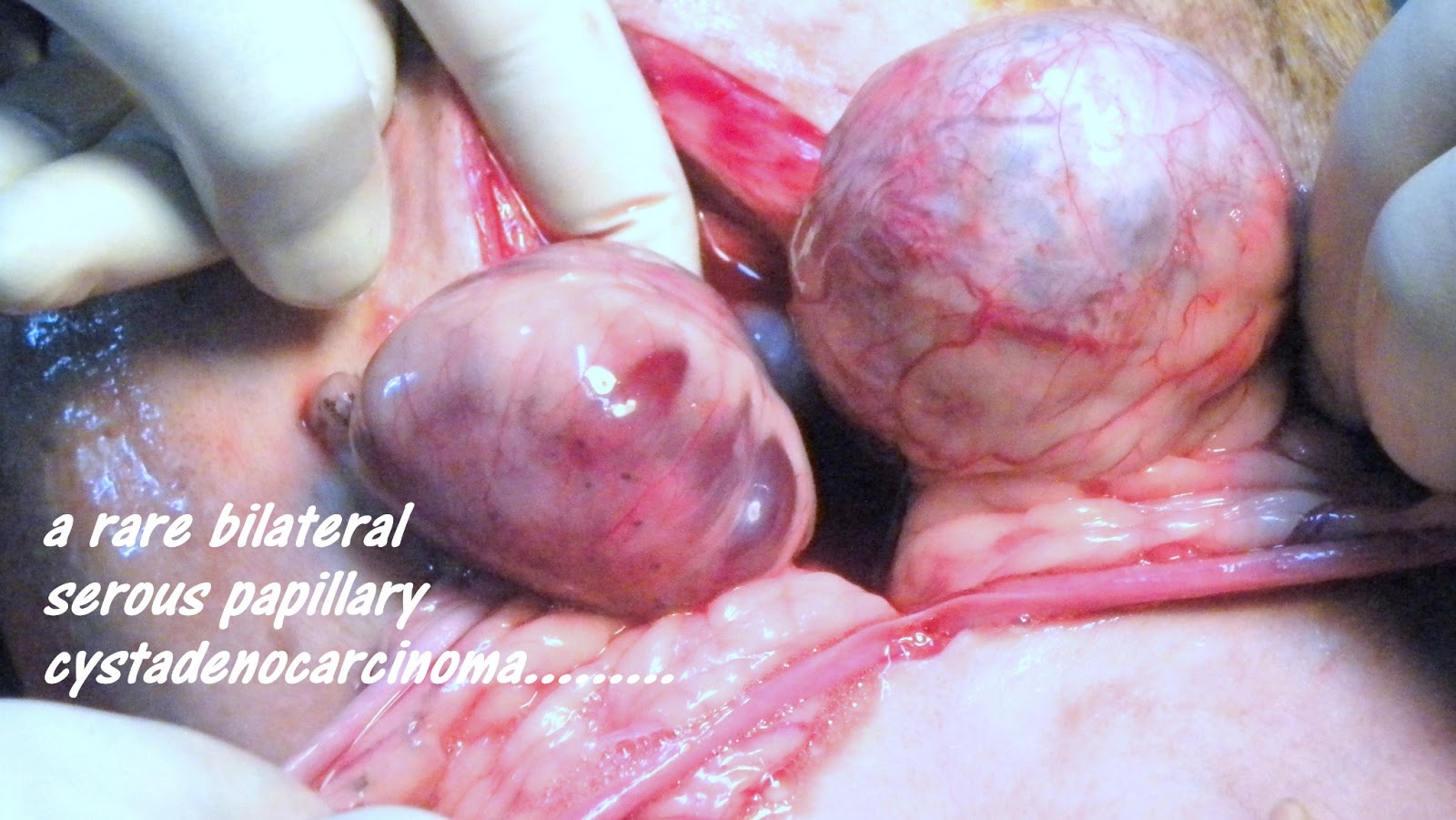
These tumours mainly include papillary adenoma,
papillary adenocarcinoma, papillary cyst adenoma and adenocarcinoma. About 40
to 60% of canine ovarian tumours fall in this category. Papillary
adenocarcinoma often is associated with widespread peritoneal invasion and
marked by malignant haemorrhagic effusion often misleading to ascites.
Development of malignant effusion is due to
i) Leakage of fluid through tumour capsule.
ii) Exfoliation of tumour cells resulting in
transcoelomic metastatic implants that exert pressure and obstruct peritoneal
and diaphragmatic lymphatics.
iii) Secretion from metastatic peritoneal implants
Papillary adenocarcinoma usually metastasizes to
kidney, liver, lungs, and omentum and par aortic lymph nodes.
Cystadenocarcinomas originate from the rete ovarii and
consists of multiple thin walled cysts.
2)
Germ Cell Tumours-
The ovarian primordial germ cells are responsible for
ovarian dysgerminomas, teratomas
and teratocarcinomas.
Dysgerminomas arise mainly from undifferentiated germ
cells and consists of ovarian primordial cells. Due to their resemblance with
testicular cells they are also called as “ovarian
seminomas”. These tumours grow by expansion and metastasis is often in
abdominal lymph nodes. However involvement of other vital organs has been also
seen.
Teratomas are mainly composed of germ cells which are
differentiated in two or more germinal cell layers. So these tumours have both
mature elements and undifferentiated elements resembling those of embryo. These
are highly metastatic in nature and it occurs in all other vital body parts.
3)
Sex Cord Stromal Tumours-
These tumours arise from the specialised gonadal stroma
of the ovary, which is responsible for oestrogen and progesterone production.
Most common sex cord stromal tumour is “Granulosa Cell
Tumour”.
These are firm, lobulated and grow quite large size,
have good metastatic potential. They are quite potential to elaborate steroid
hormones.
Alpha-inhibitin, a gonadal glycopeptides
known to be feedback inhibitor of pituitary secretion of follicular stimulating
hormone (FSH), is a useful histologic marker of Granulosa cell tumour.
The other stromal cell tumours like Thecomas and
Luteomas are also reported and are benign in nature.
Other tumours like conditions which are
found are par ovarian tumours which originate from mesonephric tubules, cystic
rete tubules, vascular haematomas and adenomatous hyperplasia of rete ovarii.
Depending upon the tissue of origin the
clinical symptoms of ovarian tumour vary. Main clinical symptom of epithelial
cell tumours is malignant ascites. Germ cell tumours are associated with
hormonal dysfunction and space occupying mass in abdomen. Routine abdominal
radiographs show enlarged mass with calcified foci. Stromal tumours secrete
steroid hormones hence excessive oestrogen hormone leads to vulvar enlargement,
sanguineous vulvar discharge, persistent oestrous, alopecia and aplastic
pancytopenia. Excessive progesterone production leads to cystic endometrial
hyperplasia/ pyometra complex.
The common diagnostic techniques are
abdominal radiography and ultrasonography. Cytological evaluation of the
malignant effusion from abdomen gives better idea.
Palliative radiation and chemotherapy
using platinum based combinations with taxanes is useful in human patients but
radical surgery remains the mainstay of treatment for ovarian tumours in
canines.
Complete ovariohysterectomy is
recommended. During surgery you have to gentle in handling tissues to minimise
transcoelomic tumour spread. Before abdominal closure careful examination of
all serosal surfaces, including omentum, diaphragm is necessary. Any suspected
lesions should be subjected to biopsy, FNAC for metastatic disease. Before
closure of abdominal incision a through wash with ample of NS is advisable.
Prognosis is very good after surgery if
no metastasis and adhesions are noticed.